Introduction
The immune system plays a vital role in protecting our body from foreign invaders. But sometimes, it can mistakenly attack our own cells. One of the best diagnostic tools that help detect such immune-related disorders, especially those affecting red blood cells (RBCs), is the Coomb’s test. Also known as the Antiglobulin Test, it helps identify antibodies or complement proteins attached to the surface of red blood cells.
This test is critical in diagnosing conditions like hemolytic anemia, Rh incompatibility in pregnancy, and reactions to blood transfusions. There are two major types of it: Direct Coomb’s Test (DCT) and Indirect Coomb’s Test (ICT). In this document, we will explore both in detail, covering their definitions, principles, procedures, clinical applications, interpretations, advantages, and limitations.
Table of Contents
What is the Coomb’s Test?
The Coomb’s test is a laboratory test used to detect the presence of antibodies that act against the surface of red blood cells. It was developed by Robin Coombs and his colleagues in 1945, which is why it’s named the Coomb’s test.
Basic Idea:
- Our red blood cells may sometimes be coated with antibodies (IgG) or complement proteins.
- These are not always visible under a microscope.
- The Coomb’s test uses an anti-human globulin (AHG) reagent to reveal these immune components.
Types of Coomb’s Test
There are two main types:
1. Direct Coomb’s Test (DCT)
Also called the Direct Antiglobulin Test (DAT).
- Detects antibodies or complement proteins directly attached to the surface of red blood cells in the patient’s body.
- Used when hemolysis (destruction of red blood cells) is suspected.
2. Indirect Coomb’s Test (ICT)
Also known as the Indirect Antiglobulin Test (IAT).
- Detects antibodies present in the patient’s serum that may bind to RBCs.
- Commonly used in blood compatibility testing and during pregnancy to detect Rh incompatibility.
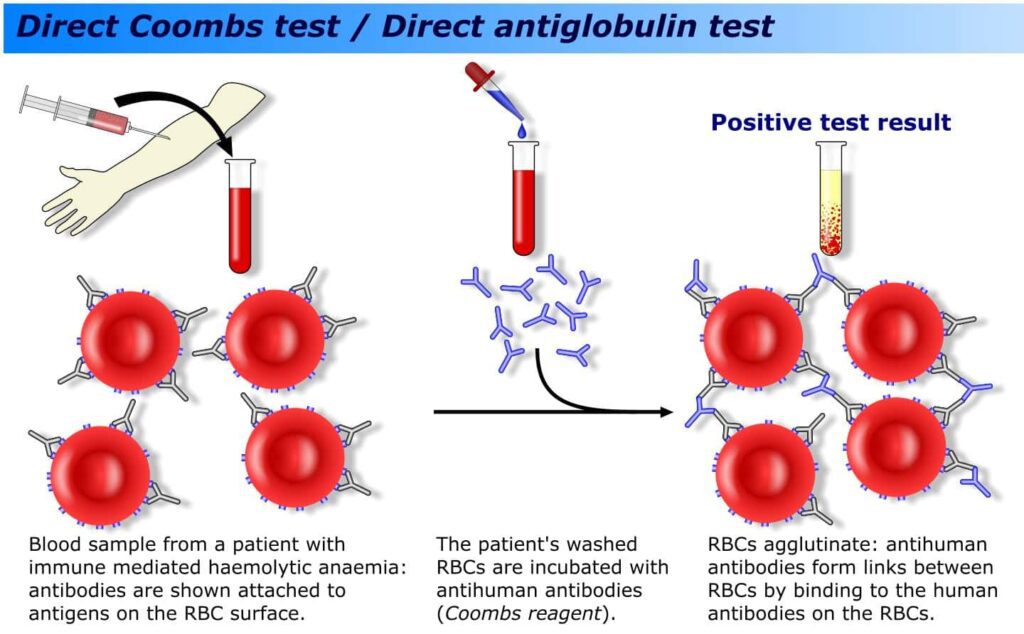
Direct Coomb’s Test (DCT)
Definition
The Direct Antiglobulin Test (DAT) is used to detect antibodies or complement proteins that are already bound to the surface of red blood cells in the bloodstream.
Principle
- Patient’s RBCs are washed to remove unbound antibodies.
- Anti-human globulin (AHG) reagent is added.
- If antibodies or complement proteins are attached to the RBCs, the AHG reagent will cause agglutination (clumping).
- Agglutination indicates a positive test.
Procedure
- Collect patient’s blood sample (EDTA-treated preferred).
- Wash RBCs 3-4 times with saline to remove unbound proteins.
- Add 1-2 drops of Coomb’s reagent (AHG).
- Gently mix and centrifuge the tube.
- Examine for agglutination under a microscope.
Clinical Applications
1. Autoimmune Hemolytic Anemia (AIHA)
In this condition, the body produces antibodies against its own RBCs.
2. Hemolytic Disease of the Newborn (HDN)
- Caused by Rh incompatibility between mother and fetus.
- Antibodies from Rh-negative mother can destroy fetal Rh-positive RBCs.
3. Transfusion Reactions
- Occurs when patient receives incompatible blood.
- Antibodies attach to transfused red blood cells.
4. Drug-induced Hemolysis
Some drugs can cause immune-mediated hemolysis.
Interpretation
| Result | Meaning |
|---|---|
| Positive | Antibodies or complement are on RBCs |
| Negative | No antibodies or complement on RBCs |
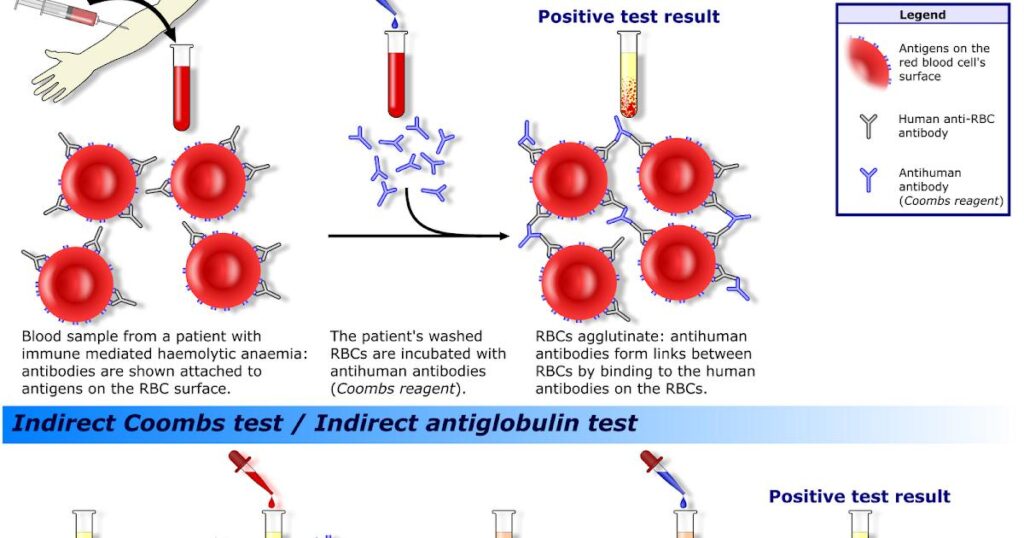
Indirect Coomb’s Test (ICT)
Definition
The Indirect Antiglobulin Test (IAT) is used to detect free-floating antibodies in the patient’s serum that can bind to red blood cells. It is commonly used in pre-transfusion testing and prenatal screening.
Principle
- The patient’s serum is mixed with reagent red blood cells (with known antigen types).
- If antibodies are present in the serum, they will bind to the RBCs.
- After incubation, Coomb’s reagent (AHG) is added.
- If agglutination occurs, the test is positive.
Procedure
- Collect the patient’s blood and separate the serum.
- Add a few drops of serum to reagent red cells.
- Incubate at 37°C for 30–60 minutes.
- Wash the mixture to remove unbound antibodies.
- Add AHG reagent.
- Centrifuge and observe for agglutination.
Clinical Applications
1. Pre-transfusion Testing
Ensures compatibility between donor and recipient blood.
2. Prenatal Antibody Screening
- Detects maternal antibodies against fetal RBCs.
- Helps manage Rh incompatibility.
3. Blood Typing and Antibody Identification
Determines presence of irregular antibodies.
Interpretation
| Result | Meaning |
| Positive | Serum contains antibodies against RBC antigens |
| Negative | No significant antibodies present |
Key Differences between Direct and Indirect Coomb’s Test
| Feature | Direct Coomb’s Test (DCT) | Indirect Coomb’s Test (ICT) |
| Detects | Antibodies or complement on RBCs | Free antibodies in serum |
| Sample used | Patient’s RBCs | Patient’s serum and reagent RBCs |
| Main use | Hemolytic anemia, HDN | Blood compatibility, prenatal testing |
| Timing | Indicates ongoing antibody binding | Indicates risk of antibody reaction |
| Agglutination caused by | Anti-human globulin + antibody-coated RBCs | Anti-human globulin + serum-bound RBCs |
Applications of Coomb’s Test in Healthcare
1. Transfusion Medicine
Ensures safe blood transfusions by detecting incompatible antibodies.
2. Pregnancy and Newborn Care
- Prevents and manages Hemolytic Disease of the Newborn (HDN).
- Allows early intervention using Rh immunoglobulin.
3. Autoimmune Diseases
Diagnoses autoimmune hemolytic anemia and other red cell disorders.
4. Drug Reactions
Some drugs can cause immune-mediated RBC destruction. Coomb’s test helps confirm diagnosis.
5. Organ Transplantation
Screens for cross-matching to avoid rejection.
Limitations of the Test
While useful, Coomb’s test has some limitations.
1. False Positives
- Overwashing RBCs or contamination may give incorrect results.
- Recent transfusions may interfere.
2. False Negatives
Insufficient washing or low antibody levels may not show agglutination.
3. Does Not Identify Specific Antibody
Only indicates presence of antibodies, not which ones.
4. Technical Errors
Requires careful temperature control and skilled handling.
Enhancing Accuracy of Coomb’s Tests
Tips:
- Ensure proper sample collection and labeling.
- Use freshly prepared reagents.
- Wash RBCs thoroughly before adding AHG reagent.
- Always include positive and negative controls.
- Repeat testing when results are ambiguous.
Recent Advances in Coomb’s Testing
1. Gel Card Technology
Uses micro-columns filled with gel for more accurate and automated detection.
2. Solid-phase Testing
Increases sensitivity and allows automation.
3. Flow Cytometry
- Offers highly sensitive detection of bound antibodies.
These methods reduce human error and improve consistency of results.
Conclusion
The Coomb’s test, both direct and indirect, remains a cornerstone in immunohematology and transfusion science. It provides essential insights into immune reactions involving red blood cells, helping diagnose serious conditions like hemolytic anemia and ensuring safe transfusions and pregnancies.
The Direct Coomb’s Test is invaluable for detecting antibodies already on red blood cells, while the Indirect Coomb’s Test plays a crucial role in anticipating potential antibody reactions before they occur.
Despite some limitations, its role in modern medicine is indispensable, especially with new automated and sensitive testing methods enhancing its reliability.
FREQUENTLY ASKED QUESTIONS
Who needs a Coomb’s test?
Patients with anemia, pregnant women (especially Rh-negative), or those undergoing blood transfusion.
Is the Coomb’s test painful?
No. It only requires a simple blood draw.
Can the test be wrong?
Yes. False positives and negatives can occur due to technical issues or biological variability.
Related Articles